
From the 1Department of Anesthesia and Critical Care Medicine, Centre Hospitalier Universitaire de Saint-Etienne, 2Univ Lyon, INSA, CNRS UMR 5520, INSERM U1206, UJM-Saint-Etienne, CREATIS, 3Department of Radiology, Centre Hospitalier Universitaire de Saint-Etienne and 4Inter-university Laboratory of Human Movement, EA7424, Univ Lyon - University Jean Monnet Saint-Etienne, Saint-Etienne, France
Objective: Muscle atrophy is frequent in critically ill patients and is associated with increased mortality and long-lasting alteration in quality of life. Muscle ultrasound has not been clearly validated in intensive care unit patients. The aim of this study was to compare the level of agreement between ultrasound and computed tomography scan for the measurement of quadriceps muscle thickness.
Design: A prospective observational study.
Patients: Forty-two consecutive patients admitted to a neurological intensive care unit.
Methods: Quadriceps thickness was measured 15 cm above the upper edge of the patella. Iterative brain computed tomography scans were associated with a quadriceps-centred acquisition sequence. Concomitantly, an ultrasound of the quadriceps was performed. The position of the studied leg was standardized for ultrasound and computed tomography.
Results: A total of 73 measurements of ultrasound and computed tomography quadriceps thickness were compared. The correlation between both measures was 0.93 (95% confidence interval (95% CI) 0.84–1.02). Intra-rater reliability of ultrasound measurements and inter-rater reliability were excellent, with an ICC of 0.98 (95% CI 0.97–0.99) and 0.96 (95% CI 0.92–0.98), respectively.
Conclusion: A specific ultrasound set-up for measurement of quadriceps thickness is reliable and reproducible in an intensive care unit population.
Key words: critical illness; muscle wasting; muscle atrophy; quadriceps muscle; ultrasonography; computed tomography scan.
Accepted Dec 10, 2019; Epub ahead of print Dec 20, 2019
J Rehabil Med 2020; 52: jrm00032
Correspondence address: Jerome Morel, Département anesthésie réanimation, Avenue Albert Raimond, 42000 Saint - Etienne Cedex. E-mail: jerome.morel@chu-st-etienne.fr
Muscle atrophy is frequent in critically ill patients and is associated with increased mortality and long-lasting alteration in quality of life. Muscle ultrasound has not been validated in intensive care unit patients. The aim of this study was to compare the level of agreement between ultrasound and computed tomography scan for the measurement of quadriceps muscle thickness. A total of 42 consecutive patients were included. Iterative brain computed tomography scans were associated with a quadriceps-centred acquisition sequence. Concomitantly, an ultrasound of the quadriceps was performed. The position of the studied leg was standardized for ultrasound and computed tomography. This study shows, for the first time in an intensive care unit population, that a specific ultrasound set-up for measurement of quadriceps thickness is reliable and reproducible.
Critically ill patients are particularly at risk of acute muscle loss. Indeed, during the first 10 days of intensive care unit (ICU) admission, patients typically present with a progressive decrease in muscle mass, amounting to a reduction of almost 20% (1). Muscle loss is associated with high morbidity and mortality (2). Long-lasting physical disabilities are also frequently reported with this syndrome, leading to altered rehabilitation and compromised quality of life (3). On the other hand, interventions that could prevent muscle wasting and restore physical capacity and mobility greatly optimize patient recovery (4). Clinicians need methods to detect muscle loss and to monitor the benefit of muscle therapies and muscle preservation.
Computed tomography (CT) scans can be considered as a reference method to study muscular anatomy (5). Ultrasound (US) is currently the easiest modality to use in an ICU. Muscle cross-sectional area (CSA) or muscle thickness (6) can be assessed by US. Studies performed in critically ill patients considered rectus femoris muscle CSA (1, 7), or thigh muscles (rectus femoris and vastus lateralis) thickness (8, 9). That said, ultrasound reliability is not clearly established (10). First, it can be difficult to delineate the whole CSA of the rectus femoris in some cases due to the limited size of the US scan window (11). Secondly, in the majority of the studies, the position of the assessed leg is not standardized. Thirdly, compression of the tissue by the probe can interfere with the measurement. We recently validated in healthy volunteers, a simple set-up and a standardized procedure to measure thigh thickness using US (12).
The aim of the current study was to validate this US set-up in critically ill neurological patients. The main objective was to measure the level of agreement between measures of thigh muscle thickness derived from US and CT imaging and the intra- and inter-observer reproducibility of US measurements.
This is a single-centre observational study. The protocol was approved by the local ethics committee and registered with Clinical Trials.gov as NCT02562495. Written informed consent was obtained from patients’ next-of-kin before study enrollment.
Subjects
Consecutive patients (n = 42) admitted to our neurological ICU were prospectively included if they presented a Glasgow score ≤ 8 at admission, required mechanical ventilation, and if patients were a priori scheduled for iterative follow-up brain CT scans. A maximum of 3 CTs was used in the study during the 10 first days of admission. Patients were excluded if they presented a bilateral leg injury, or morbid obesity (body mass index > 35 kg/m2).
Ultrasound and computed tomography acquisitions
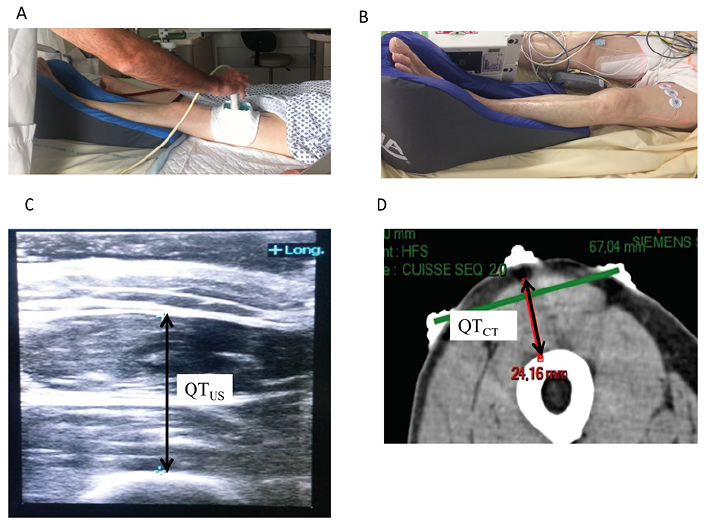
In order to carefully standardize positioning of the leg and muscles for both US and CT procedures, all subjects were examined in a strict supine position. The right leg was positioned into a foam device maintaining the feet in an upright position (Fig. 1A and 1B). For muscle thickness measurement the level of interest was localized 15 cm above the upper edge of the patella, perpendicular to the patella; anterior - superior iliac spine axis. A landmark was drawn on the skin with a permanent marker to ensure reproducibility across modalities and measurements.
A CX50x MATRIX ultrasound system (Philips, Amsterdam, The Netherlands) equipped with a linear transducer (Philips, L12–4; 34 Hz) was used for all measurements. Special care was taken not to induce any pressure on the analysed muscles, while preserving optimal coupling of the probe during measurement. Therefore, a custom-made system was developed to enable precise and ergonomic positioning of the transducer (Fig. 1A). All measurements were undertaken, while always maintaining a 1-cm ultrasound gel layer between the transducer and the skin, ensuring no compression of the transducer.
CT imaging was performed on a Siemens Somatom Definition AS64 unit (Siemens, Erlangen Germany). Patients were installed in a decubitus position with the leg positioned via the same protocol described for the US protocol (Fig. 1B). Three radio-opaque electrodes were placed along the landmarked skin; 1 on the axis of the leg and 2 on each side (Fig. 1B). CT-scout view was centred on the radio-opaque markers for slice location acquisition. The mean additional radiation burden was 0.03 mSv.
The maximum time delay between US and CT acquisitions was less than 1 h.
Ultrasound and computed tomography evaluation protocol
Ultrasound quadriceps thickness (QTUS) measurements were defined as the distance between the upper border of the femoral bone and the lower boundary of the subcutaneous tissue, incorporating both the rectus femoris muscle and the vastus intermedius muscle (Fig. 1C).
Inter-rater reliability was assessed by asking 2 independent and blinded practitioners to carry out QTUS on the same patients, in a similar environment, and within a 1-h delay. Measurements were repeated 3 times by each operator in order to determine intra-rater reliability assessments. To avoid a recall bias, repeated measures were always started from the baseline, with the transducer initially placed in its storage compartment. Individual measures were averaged when comparing US and CT measurements.
Fig. 1. Ultrasound (US) and computed tomography (CT) positioning and measurement protocols. (A) Leg positioning during US procedure. To ensure that no pressure was exerted during measurement by the transducer itself, a flexible silicon “pool” was designed, conforming to the anterior thigh while maintaining an ultrasound gel layer between the transducer and the skin. (B) Leg positioning during CT procedure. Three radio-opaque electrodes were placed along the landmarked skin; one on the axis of the leg and 2 on each side. CT-scout view was centred on the radio-opaque markers for slice location acquisition. (C) Measurement of US quadriceps thickness (QTUS). QTUS was the distance between the upper border of the femoral bone and the lower boundary of the subcutaneous tissue. (D) Measurement of CT quadriceps thickness (QTCT). We first drew the line passing through the 2 external electrodes. We then drew the perpendicular passing through the central electrode and the femoral bone. QTCT was measured on this line and followed the same protocol as previously described for US.
Sample size
Sample size was calculated from an estimation of the 95% confidence interval (95% CI) of the mean difference observed between both techniques (limit of agreement). The number of patients to be included was 38 (see Supplementary information1 for more details).
Statistical analysis
Data were initially screened for normality using the Shapiro–Wilk test, and were accordingly reported as mean (standard deviation (SD)) or median and 95% CI.
Intra-rater and inter-rater reliability were calculated using an intraclass correlation coefficient (ICC) (2,1) 2-way random consistency model. An ICC greater than 0.8 was indicative of an “almost perfect” agreement. We also calculated the standard error of measurement (SEM) using the following formula: SE = SD × (1–ICC), where SD is the global SD of measurements, and the minimum detectable change (MDC) estimated on a 95% CI, where MDC = 1.96 × SEM.
The agreement between QTUS and QTCT was analysed using the non-parametric Passing-Bablock analysis procedure after a CUSUM test for linearity validation, and a Bland-Altman plot with limits of agreement calculation. For all analyses, statistical significance was accepted at p < 0.05.
A total of 42 patients were enrolled from August 2015 to December 2016, 4 patients were excluded due to unusable images (either US or CT). The first evaluation was performed 24 h (SD 12 h) after admission, 25 patients (65.8%) had a second evaluation 3.2 days (SD 1.3 days) after admission and 10 (26.3%) had a third evaluation 6.6 days (SD 3.6 days) after admission.
Intra- and inter-rater reliability of ultrasound quadriceps thickness measurement
Intra-rater reliability of US measurements was excellent, with an ICC of 0.98 (95% CI 0.97–0.99). SEM was 0.06 cm and the minimal detectable change (MDC) was therefore 0.12 cm. Inter-rater reliability was also excellent, with an ICC of 0.96 (CI 95% 0.92–0.98). SEM inter-rater was 0.106 cm, translating to a MDC of 0.21 cm.
Agreement between ultrasound quadriceps thickness and computed tomography quadriceps thickness for the measurement of quadriceps muscle thickness
Passing-Bablock regression showed no significant deviation from linearity (CUSUM test, p = 0.37). There was no significant systematic difference between US and CT measures, with an intercept A equal to 0.089 (95% CI –0.14–0.27) and no significant proportional differences, since the slope was 0.93 (95% CI 0.84–1.02) (Fig. 2A). Bland-Altman analysis showed a 0.097 cm mean bias for measurements (95% CI 0.04–0.14), with upper and lower limits of agreement of 0.55 (95% CI 0.46–0.63) and –0.356 (CI 95% –0.44 –0.26), respectively (Fig. 2B). The coefficient of repeatability was 0.48 (95% CI 0.42–0.57).
Fig. 2. Comparison of quadriceps thickness measurement with ultrasound (US) (QTUS) and computed tomography (CT) scan (QTCT). (A) Passing & Bablok analysis with the linear regression line (blue line) and its 95% confidence interval (95% CI). (B) Bland-Altman analysis. The bias (continuous blue line) with its 95% CI.
This study showed that, in critically ill neurological patients at risk of developing intensive care unit-acquired weakness, a protocol of US quadriceps muscle thickness measurement ensuring no compression during measurements has an excellent intra-rater (ICC = 0.98) and inter-rater (ICC = 0.96) reliability. In addition, compared with CT measures, no systematic or proportional difference and a bias of less than 0.1 cm
was found. From a practical point of view, when multiple measures are performed by different raters with US, the minimal detectable difference (MDCUS) was 0.21 cm, meaning that any difference of at least
0.21 cm can be considered to be real.
In patients with coronary artery disease, Thomaes et al. found a limit of agreement of 0.01 cm (SD 0.24 cm) between US and CT (13). ICU patients present specific characteristics, particularly in the acute phase, such as an important subcutaneous oedema and, frequently, a general anaesthesia, which both complicate the analysis of the muscle. However, a validated tool is essential to measure muscle mass in ICU patients and to evaluate rehabilitation strategies. To the best of our knowledge, this is the first study validating an US muscle protocol in critically ill patients.
Several studies analysed muscle mass in critically ill patients through muscle CSA (1), or quadriceps muscle thickness (14). Since the wasting process is probably not uniform across muscles (15), some authors propose measuring global muscle thickness, calculated as the mean, across a variety of muscle groups (7). All except one study, but with a high loss of follow-up, report a decrease in muscle mass (14). The rate of muscle wasting varies greatly among studies, ranging from 1.6% to 6% per day (6, 7), with more notable wasting in patients with greater muscle thickness at baseline (7) and those with multiple organ failure (1). One study measured both rectus femoris thickness and CSA. The parameters were not directly compared, but their kinetics across the first 10 days of ICU admission were similar (15). In another study, US underestimated muscle waste, as shown by a 10.3% decrease in rectus femoris CSA with US from day 1 to day 7, while the decrease was 17.5% with the fibre cross-sectional area (1).
In ICU patients, muscle US is reproducible with high inter- (1) or intra-observers agreement (8). A low inter-observer agreement has been pointed out in one study (10). The standardization of the studied leg position and the US technique with minimal probe compression probably explain our high intra- and inter-observer agreement.
Muscle ultrasound: a surrogate for lean body mass or whole muscle mass
Muscle is the largest store of lean mass and constitutes approximately 40% of lean body mass. In healthy volunteers, muscle thickness correlates significantly with lean body mass (16). The sum of muscle thicknesses at different sites improved this correlation (6). In ICU patients, thigh muscle thickness was moderately correlated with the muscle cross-section area of the third lumbar vertebra determined by CT scan, a reliable marker of skeletal muscle mass (15).
Muscle ultrasound: a surrogate for muscle function
Strength correlates with muscle thickness or rectus femoris cross sectional area (RF CSA) in healthy volunteers or clinical populations (13). This correlation is not established for critically ill patients. When normalized to fat-free body mass, the pattern of muscle thickness assessed 16 days after ICU admission differed from that of muscle weakness (15). Others report a weak to moderate correlation between thickness and volitional strength testing (15). These results suggested that factors other than wasting account for strength loss, and that muscle size may not be an appropriate surrogate measure of strength. Ideally, a simultaneous measurement of strength via nerve stimulation and muscle mass would validate the correlation between both parameters in critically ill patients. This aspect has not yet been investigated in ICU patients.
Limitations
This study focused on critically ill neurological patients, and the results may be different in other ICU populations. We chose to measure the thickness of the thigh, because wasting seems to be more marked compared with other muscles groups, and the quadriceps group may also have greater implications compared with other muscle groups depending on the outcome, such as ICU length of stay and physical function at ICU discharge (15). Therefore, conclusions might be different in other muscle groups.
Conclusion
The current findings suggest that the protocol used in this study has the potential to become a useful tool to assess quadriceps thickness at the bedside and could help to extend the clinical applicability of US in ICU patients. Further studies are needed to establish the correlation between muscle thickness and outcomes.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize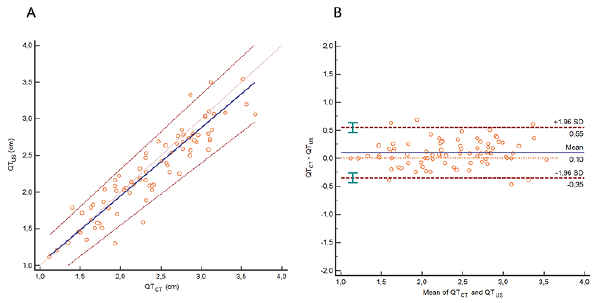 Click to show fullsize
Click to show fullsize